Foreskin Restoration
18 January 2026 Kim Jin Hong MD PhD
Single Stage Surgery
Two Stage Surgery
There are many established techniques for using regional fasciocutaneous flaps in reconstructive surgery across various parts of the body. A fasciocutaneous flap is a type of composite flap that includes skin, subcutaneous tissue, and the underlying fascia, all supplied by a consistent vascular network (fasciocutaneous perforators).
Peno-Scrotal flaps are a valuable and frequently used technique for penile and urethral reconstruction due to the scrotum's excellent vascularity, thin and elastic skin, and the genito-pudendal nerve distribution matches the genital region well. The design is based on the specific vascular supply of the area.
Scrotal Advancement Flaps which starts from the ventral aspect of the penile skin
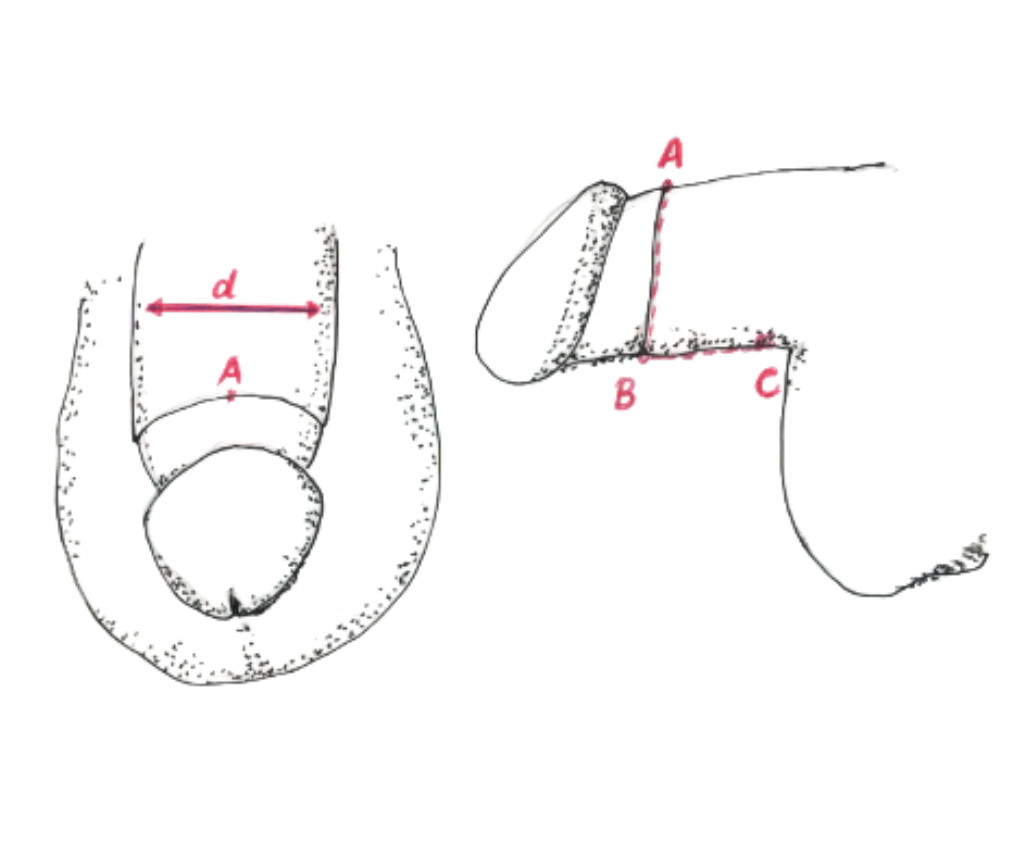
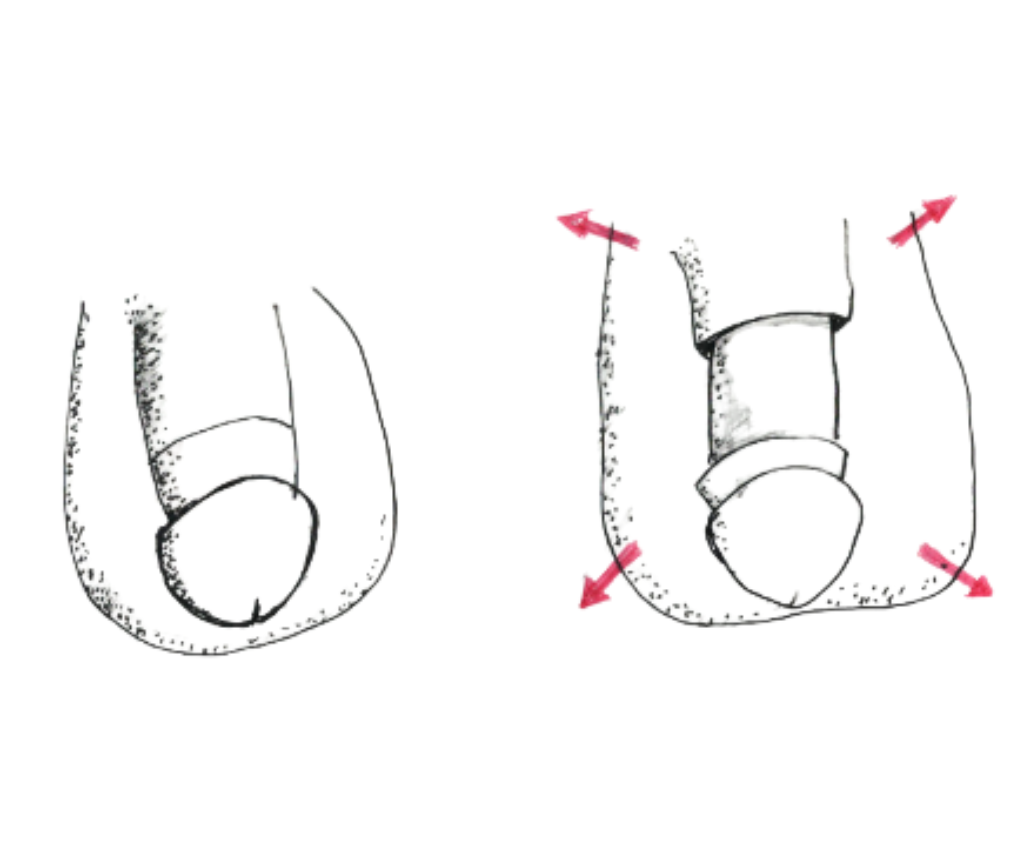
For smaller defects in the adjacent area, direct advancement of local scrotal tissue can be performed. This is feasible when the desired foreskin restoration is up to 6cm.
Scrotal flap techniques offer durable and highly effective options for genitourinary reconstruction, leveraging the unique properties of the local tissue.
Used to cover significant penile skin defects caused by trauma, infection (like Fournier's gangrene), or foreign body injections.
18 January 2026 Kim Jin Hong MD PhD
Single Stage Surgery
Two Stage Surgery
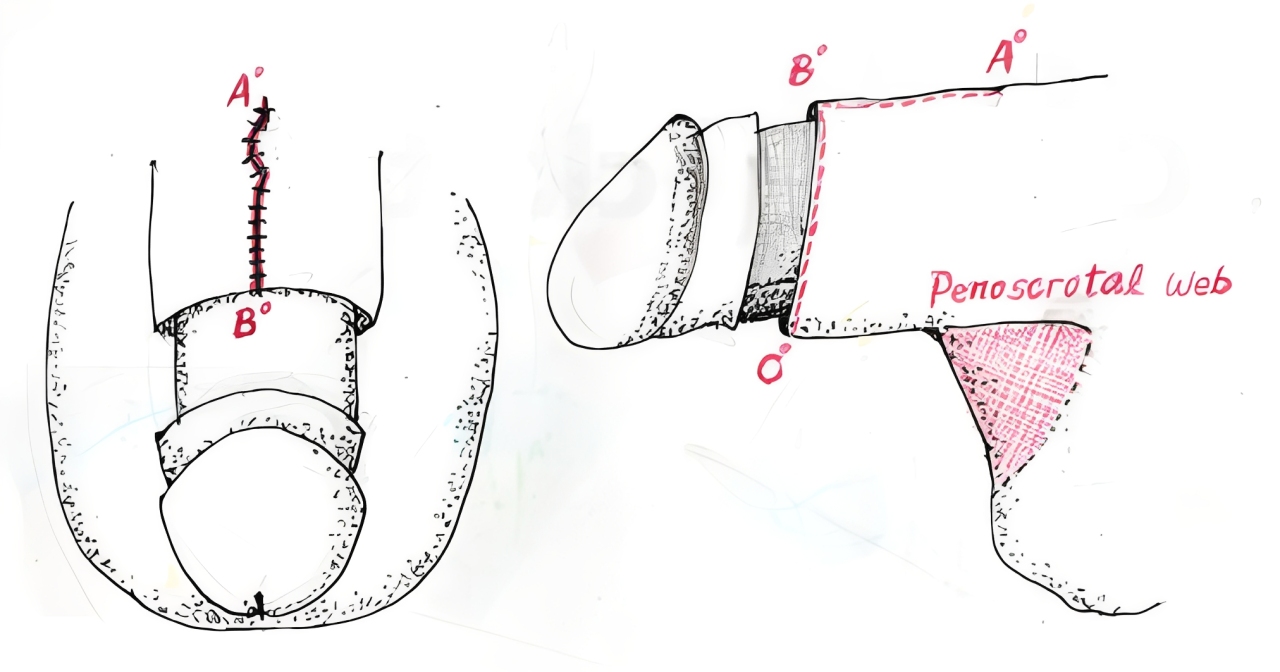
by using mobilization of the Regional Peno-Scrotal Flap together with subsequent Penoscrotal-Web correction

For the treatment of trapped penis problem that is secondary to:
The benefits of regional flap techniques are:
When the desired gap of penile skin length is less than 6 cm, it is advisable to choose single stage procedure.
Case One
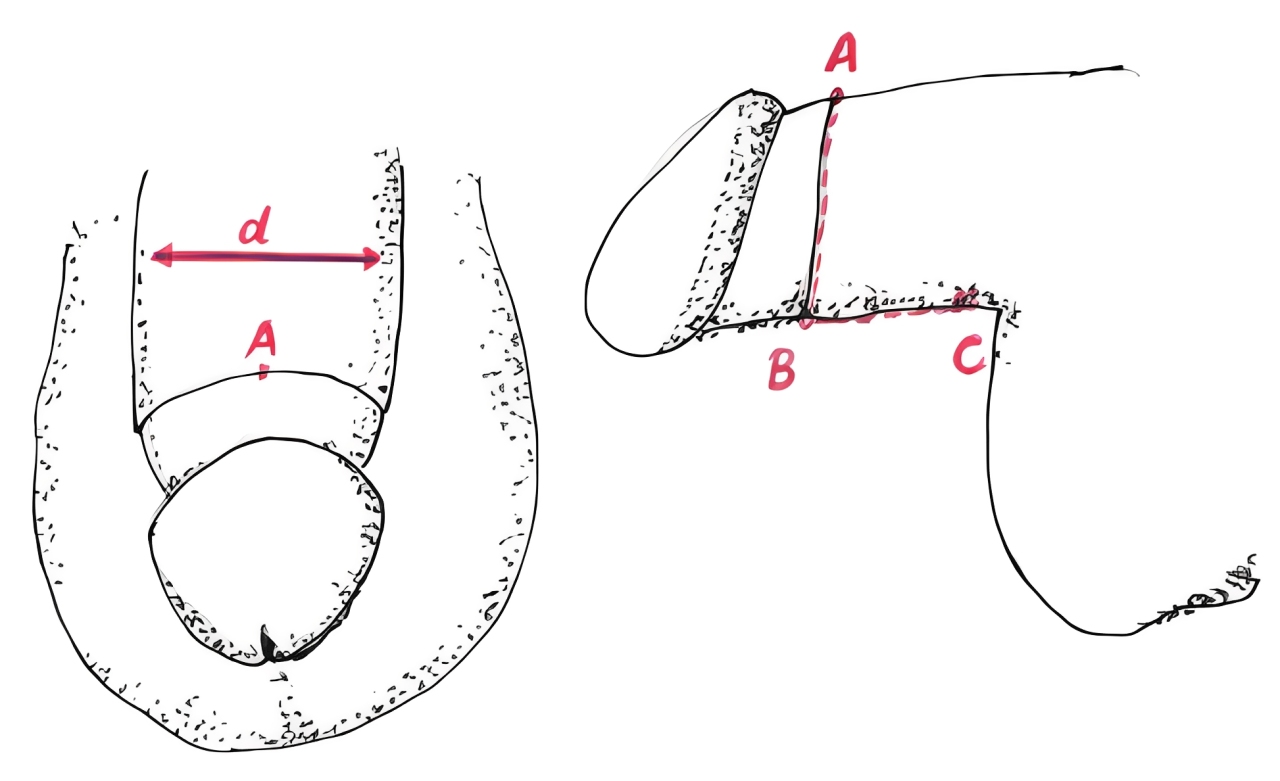
This patient was 32 years old, 172 cm tall, and weighed 118 kg. He had been circumcised at the age of 12. He experienced long-term dissatisfaction with his body image. His penile length was 11 cm and girth was 12 cm during full erection. The pre-calculated expected gain was half the girth length using a single-stage surgical procedure — approximately 6 cm gain.
When the desired gain of penile skin length exceeds 6 cm, it is advisable to achieve the result in two stages, or select a composite flap design to enable a single-stage surgery using an extended scrotal flap.
Case Two
The featured 52-year-old patient had undergone neonatal circumcision and experienced a shortage of penile skin, causing pressure on the penile shaft during full erection. Over time, this led to ventral scrotal and dorsal pre-pubic webbing.
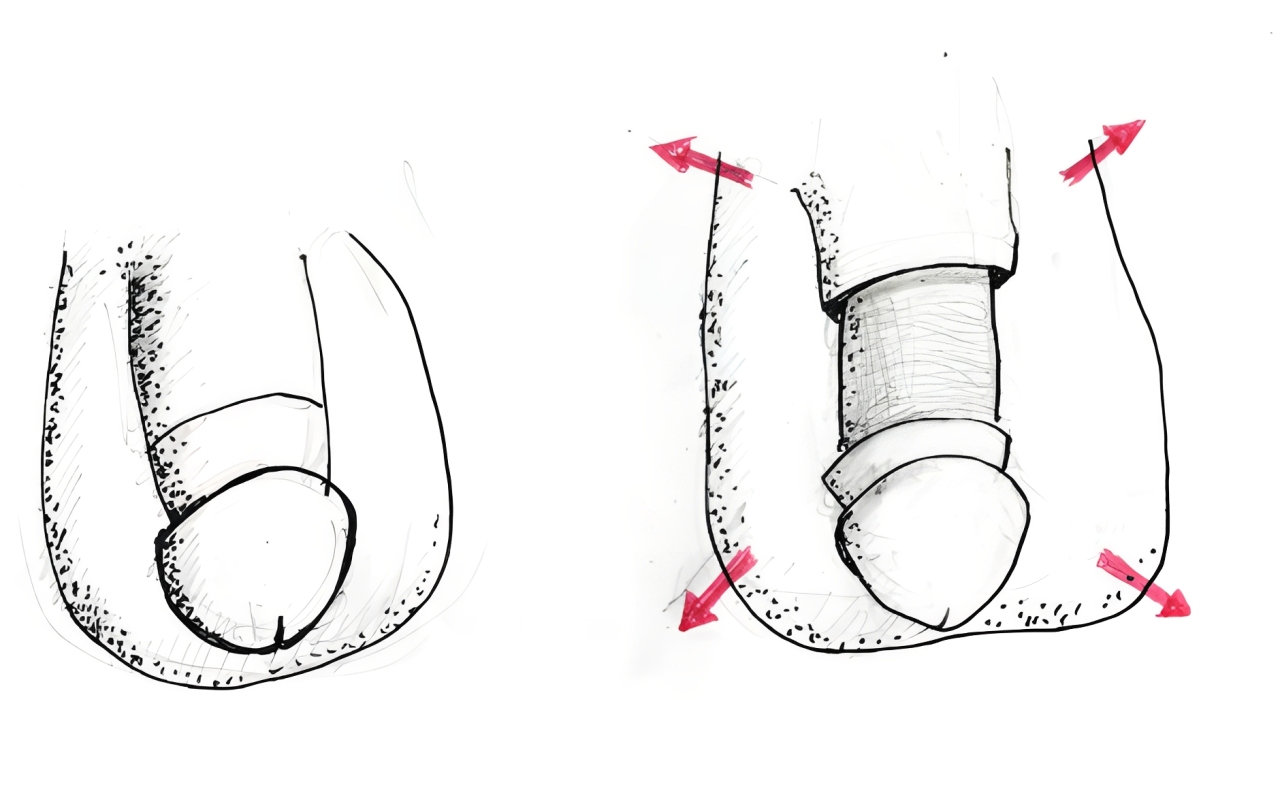
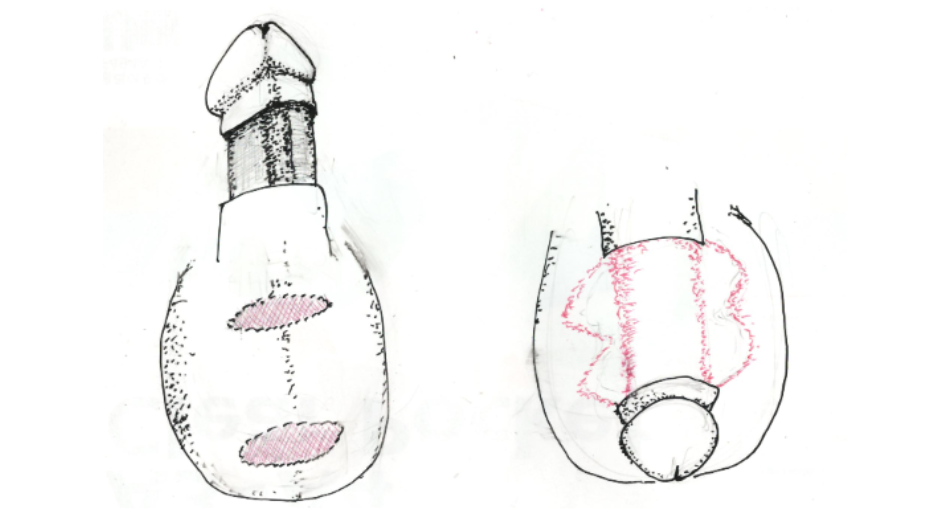
As he preferred to keep all native penile skin in its original position, he opted for a two-stage surgical procedure. This involved embedding the penile shaft into the anterior scrotum after degloving, followed by tissue separation six months later. These procedures can be performed under local anesthesia with sedation, spinal anesthesia, or general anesthesia, depending on patient preference.

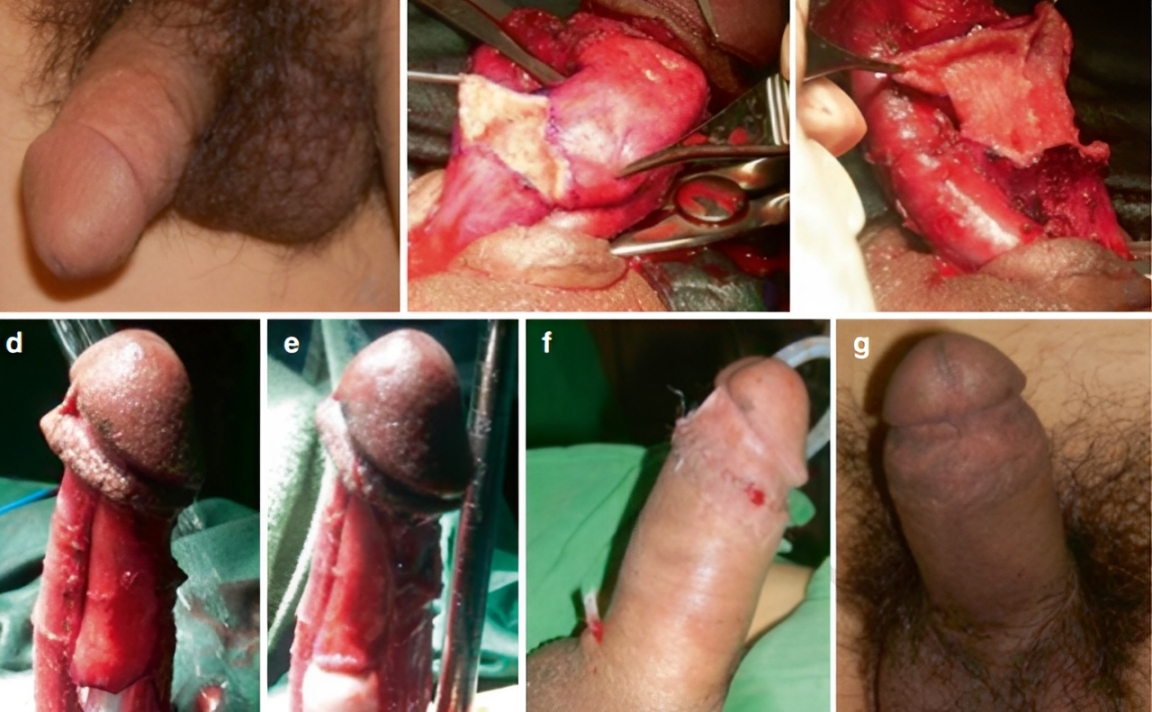
Case Three
The healthy 47-year old patient suffered from trapped penis secondary to neonatal circumcision. His shortage of penile skin was much more serious than Case 1.
In this challenging case, it was most advisable to choose spinal or general anesthesia rather than local anesthesia, because of the long operation time and the wide area of the surgical fields.
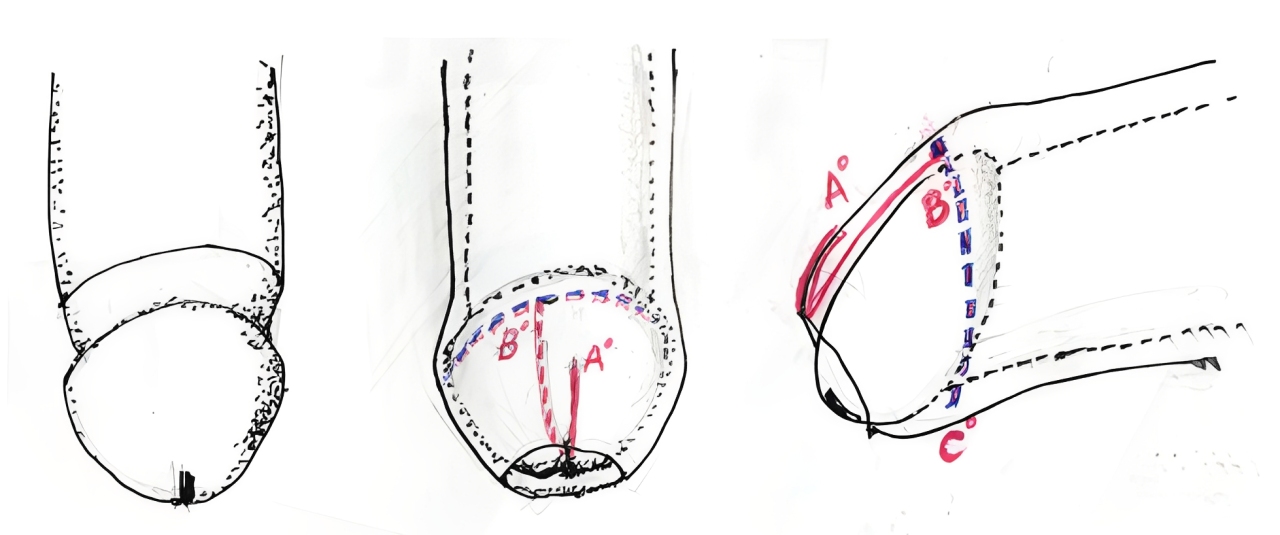
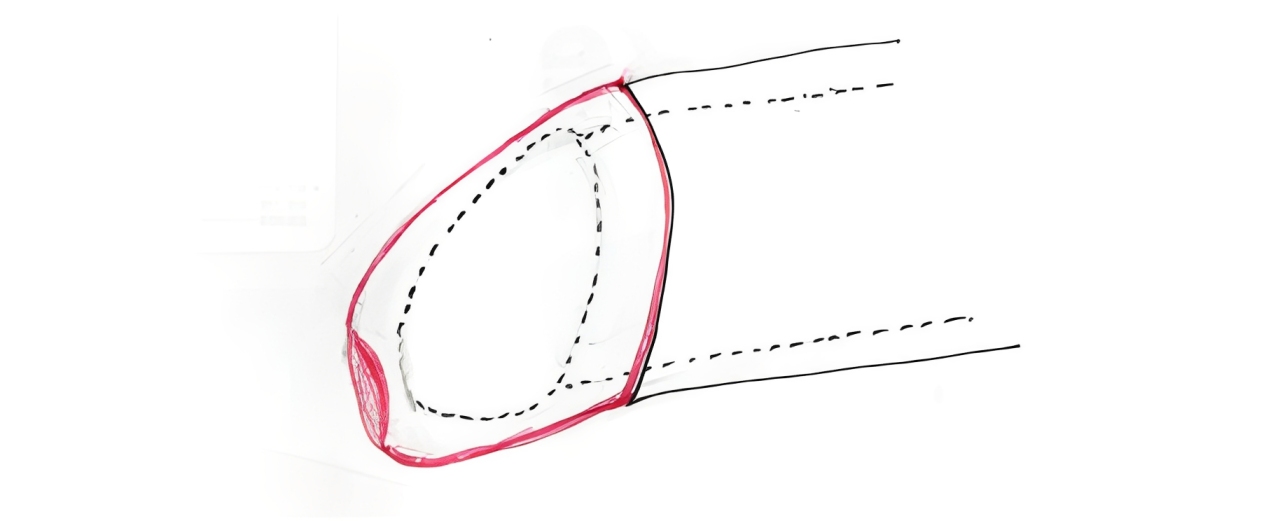
The surgical design for him was harvesting three discrete flaps from the hairless part of the scrotum and reassemble them at the distal part of the penile shaft at the circumcision line. We can finish the surgery within a single stage but it requires six hours of surgery epidural anesthesia.